I have blogged about this before. If you could do a genetic test to find out if you are likely to get an ailment and die of it, would you want to know?
I am still up in the air on this one. I was interested to read about a 21 year old woman who has the BRCA 1 gene, watched her mother die of cancer, but has decided she doesn't want to know. Her choice is to live an unstressed like without the burden of the knowledge that she could die of cancer and what it would be like.
I can completely understand that point of view. Just because we can learn about our medical and genetic make up, do we have to learn it? I mean is there a benefit to living in ignorance and letting life happen around us with out having to learn what might or might not happen to us?
Why are we supposed to learn to see what the future brings? I have never been to a palm reading or a fortune teller or anything. I haven't really wanted to. Isn't it better to have life unfold as it may than to plan and learn and change ourselves to compensate for what we learn?
Hindsight in light is always 20/20 - we always look back and think back how we could have done better or differently or improved the outcome. But is it really to our benefit to think how we might have done things differently? Then we spend too much time ruing our decisions.
This would complicate my life immensely. If I knew then I would have too much time to over plan my life which would cause me to spend time ruing my decisions and over thinking everything.
I don't want to know.
Monday, December 31, 2012
Sunday, December 30, 2012
Good bye 2012, Hello 2013 health care-wise
So if you read CNN, which I do. I find it much easier than watching CNN - either HLN screaming about new 'factoids' and miracles, or regular CNN going on and on and on about something boring and political that will put me to sleep before I learn anything. I prefer my news in the low brow way - tell it like it is and keep it short. This is why I like CNN online - because I can skip through articles instead of listening to people S L O W L Y reading them. I don't have a lot of time in my life to waste on the news. I have better things to do - like have fun.
I have digressed. CNN put out their list of the top health news stories of 2012 - which I found to be exceptionally lame as several of them focus on individual people. Here's the list:
But here is the list for 2013 of things to look out for:
I have digressed. CNN put out their list of the top health news stories of 2012 - which I found to be exceptionally lame as several of them focus on individual people. Here's the list:
- Supreme Court upheld the Affordable Care Act.
- Woman from Georgia and her case of flesh eating bacteria
- Meningitis from steroid injections that killed 39
- The Record West Nile Virus outbreak
- Robin Roberts bone marrow transplant
- Hantavirus at Yosemite
- Jesse Jackson and bi-polar disorders
- Spike in autism cases
- Kathy Bates double mastectomy
- Hepatitis C from the traveling hospital worker
But here is the list for 2013 of things to look out for:
- Medicaid expansion
- Medicaid provider payments will go up so more providers will take medicaid patients
- Health insurance exchanges
- Medicaid taxes are going up for those making over $250,000
- Medicare reform
- Insurance transparency - health insurance policies will need to be understandable
- Health care spending will be a big issue
Saturday, December 29, 2012
Recent blog posts suck
Okay, I admit my recent blog posts suck. I have been busy. I have been sleeping. I have been working. We have house guests. Its the holidays. But my blog posts have sucked for longer than just this past week or so. I am not as inspired or as inspiring I guess.
The main reason for not having as much to say is because my cancer stuff seems to be falling more in the background. Which is a good thing. But its not that it has fallen in the background but that my other health issues are overtaking the cancer crap. Currently. I am sure my cancer crap will return to the forefront and upcoming doctor appointments. In some ways its nice to have multiple medical ailments because I can alternate my stress.
My recent doctor appointments have all been about my back and RA and fibro. But I have upcoming appointments in the next month or so on my back and RA and fibro where I can discuss how treatment is going and what are we going to do to change it, and alternatives, and all sorts of fun things.
But I also have upcoming appointments in the next month or so with oncologists and endocrinologists (with thyroid cancer you get an endo instead of an onc most of the time). These conversations will be cancer related so I'll be able to stress about cancer again.
I need some time to find our more about some research which is new and exciting but the news these days is all about the stupid politican's cliff.
I digress. My recent blog posts suck. I will work on them and attempt to be inspired more in the future.
The main reason for not having as much to say is because my cancer stuff seems to be falling more in the background. Which is a good thing. But its not that it has fallen in the background but that my other health issues are overtaking the cancer crap. Currently. I am sure my cancer crap will return to the forefront and upcoming doctor appointments. In some ways its nice to have multiple medical ailments because I can alternate my stress.
My recent doctor appointments have all been about my back and RA and fibro. But I have upcoming appointments in the next month or so on my back and RA and fibro where I can discuss how treatment is going and what are we going to do to change it, and alternatives, and all sorts of fun things.
But I also have upcoming appointments in the next month or so with oncologists and endocrinologists (with thyroid cancer you get an endo instead of an onc most of the time). These conversations will be cancer related so I'll be able to stress about cancer again.
I need some time to find our more about some research which is new and exciting but the news these days is all about the stupid politican's cliff.
I digress. My recent blog posts suck. I will work on them and attempt to be inspired more in the future.
Friday, December 28, 2012
My daily nap
I have never been one for taking naps. I mean probably since I turned 3 I haven't been much of a napper. There was one semester in college where I found a daily nap meant I could stay out late at the campus bar, make it to my early classes at the same time, and keep my grades up. But I was also young then. During chemo, I did become a fan of napping for a while but then I got past that. And those naps were chemically induced shall we say.
Now I have again learned about the benefits of my daily nap. When possible I seem to fit in a daily nap of 2 hours or so if I can. Even if I go to bed early I still need my daily nap.
This is a side benefit of rheumatoid and fibromyalgia. I call it a benefit because my cat appreciates the daily nap as well.
There are people who do not understand my need for sleep and rest these days. Its not going to change anytime soon. Nor is it possible to work up to staying up and not requiring sleep. Evening events are tough for me, not that I have ever been much of a night owl but now you can pretend I'm either 2 and need a daily nap or 90 and need a daily nap.
For now, I need my sleep. There is hope I will get past this at some point but I'm not so sure.
Now I have again learned about the benefits of my daily nap. When possible I seem to fit in a daily nap of 2 hours or so if I can. Even if I go to bed early I still need my daily nap.
This is a side benefit of rheumatoid and fibromyalgia. I call it a benefit because my cat appreciates the daily nap as well.
There are people who do not understand my need for sleep and rest these days. Its not going to change anytime soon. Nor is it possible to work up to staying up and not requiring sleep. Evening events are tough for me, not that I have ever been much of a night owl but now you can pretend I'm either 2 and need a daily nap or 90 and need a daily nap.
For now, I need my sleep. There is hope I will get past this at some point but I'm not so sure.
Thursday, December 27, 2012
My goals
Now these are not by any stretch New Year's Resolutions - that isn't until next week so I have lots of time left to procrastinate on them. These are goals of things I want to do. I mean besides win the lottery or find the cure for cancer and stuff like that. These are just some basic goals.
I have been reading other people's blogs for as long as I have been blogging. Most of them are written by other cancer people. I also hang out online with all sorts of healthy and unhealthy people. I have learned a lot about how people regard life with their ailments. I know what I think but sometimes I am a slacker.
Okay, here they are:
I have been reading other people's blogs for as long as I have been blogging. Most of them are written by other cancer people. I also hang out online with all sorts of healthy and unhealthy people. I have learned a lot about how people regard life with their ailments. I know what I think but sometimes I am a slacker.
Okay, here they are:
- I will not succumb to the 'woe is me' attitude. So I had cancer twice now (and am still here) but it is not a case of woe is me. I will prevail.
- Cancer is not going to kill me anytime soon. I don't care what stage you are, your cancer is not necessarily what is going to kill you. You could get hit by a bus tomorrow just like anyone else. If you are Stage IV, it is still true for you - a bus could come your way. So why live like cancer is what is going to do you in? And with treatment these days, there are people living out there for decades with metastases. So my goal is to live as long as possible.
- There is a lot more to life than my list of ailments and boxes of pills and doctor appointments. I can't do some of the things I used to be able to do - like skiing off the top of the headwall into a big bowl of powder snow, or climb big mountains, or whatever. But I still can do a lot of things and have fun doing it.
Wednesday, December 26, 2012
Go P53! Rah Team P53!
[But before I begin this morning you will note the little new badge to the right-->
where you can vote for my blog for one of the best breast cancer blogs of 2012. Click on the little link and then find my blog and vote for it. When I last checked it was on the top of page 6 when sorted alphabetically. I have no votes yet so I'm feeling a little lonely - but it only started yesterday.]
Anyhow we are on Team P53 now. Here's a bit of an explanation of who P53 is and why we want to be on their team:
"Normal healthy cells have a mechanism that tells them to die if their DNA is too badly damaged to repair. Cancer cells have grotesquely damaged DNA, so ordinarily they would self-destruct. A protein known as p53 that Dr. Gary Gilliland of Merck calls the cell’s angel of death normally sets things in motion. But cancer cells disable p53, either directly, with a mutation, or indirectly, by attaching the p53 protein to another cellular protein that blocks it. The dream of cancer researchers has long been to reanimate p53 in cancer cells so they will die on their own."
P53 has been known about for about 20 years. It was Science Magazine's (don't laugh) Molecule of the Year in 1993 and even had the cover for a month. (Really! So its already cool so we want to be on its team.)
It was also called, in an editorial, “a cure of a terrible killer in the not too distant future.” So even its hero status has been known for a long time. This is the Joe Namath-Bobby Orr-Yogi Berra-Neil Armstrong-Nelson Mandela-Mick Jagger-Winston Churchill-Dr Salk-Mother Theresa MVP of the year protein. We want to be on the team P53.
Right now there are three drug companies - Merck, Sanofi, and Roche - about to begin testing a new drug each that will work on a wide variety of cancers - breast, lung, prostate, and liver - that will work with P53 to help reanimate it so the cancer cells die off.
"Great uncertainties remain, but such drugs could mean new treatments for rare, neglected cancers, as well as common ones. Merck, Roche and Sanofi are racing to develop their own versions of a drug they hope will restore a mechanism that normally makes badly damaged cells self-destruct and could potentially be used against half of all cancers"
So the thought is that in the future, the organ where the cancer is based will become less important than its molecular make up.
This will have a very significant impact on a range of issues related to cancer. One result, the philanthropy and awareness efforts surrounding different types of cancer will shift their goal and pool their resources. Groups that now focus on a single type of cancer, such as the Komen-for-a-Cure pink cult will become a way of the past (and we never thought we could get rid of them) as research is pooled and focus on the genes and molecular impact. So team P53 will not even have pink cheerleaders.
I'm all for Team P53 here. Please join me.
You can read the full article here.
where you can vote for my blog for one of the best breast cancer blogs of 2012. Click on the little link and then find my blog and vote for it. When I last checked it was on the top of page 6 when sorted alphabetically. I have no votes yet so I'm feeling a little lonely - but it only started yesterday.]
Anyhow we are on Team P53 now. Here's a bit of an explanation of who P53 is and why we want to be on their team:
"Normal healthy cells have a mechanism that tells them to die if their DNA is too badly damaged to repair. Cancer cells have grotesquely damaged DNA, so ordinarily they would self-destruct. A protein known as p53 that Dr. Gary Gilliland of Merck calls the cell’s angel of death normally sets things in motion. But cancer cells disable p53, either directly, with a mutation, or indirectly, by attaching the p53 protein to another cellular protein that blocks it. The dream of cancer researchers has long been to reanimate p53 in cancer cells so they will die on their own."
P53 has been known about for about 20 years. It was Science Magazine's (don't laugh) Molecule of the Year in 1993 and even had the cover for a month. (Really! So its already cool so we want to be on its team.)
It was also called, in an editorial, “a cure of a terrible killer in the not too distant future.” So even its hero status has been known for a long time. This is the Joe Namath-Bobby Orr-Yogi Berra-Neil Armstrong-Nelson Mandela-Mick Jagger-Winston Churchill-Dr Salk-Mother Theresa MVP of the year protein. We want to be on the team P53.
Right now there are three drug companies - Merck, Sanofi, and Roche - about to begin testing a new drug each that will work on a wide variety of cancers - breast, lung, prostate, and liver - that will work with P53 to help reanimate it so the cancer cells die off.
"Great uncertainties remain, but such drugs could mean new treatments for rare, neglected cancers, as well as common ones. Merck, Roche and Sanofi are racing to develop their own versions of a drug they hope will restore a mechanism that normally makes badly damaged cells self-destruct and could potentially be used against half of all cancers"
So the thought is that in the future, the organ where the cancer is based will become less important than its molecular make up.
This will have a very significant impact on a range of issues related to cancer. One result, the philanthropy and awareness efforts surrounding different types of cancer will shift their goal and pool their resources. Groups that now focus on a single type of cancer, such as the Komen-for-a-Cure pink cult will become a way of the past (and we never thought we could get rid of them) as research is pooled and focus on the genes and molecular impact. So team P53 will not even have pink cheerleaders.
I'm all for Team P53 here. Please join me.
You can read the full article here.
Tuesday, December 25, 2012
Happy Holidays
Merry Christmas, Happy New Year, Happy Kwanzaa, Happy Festivus, Happy Hanukkah and whatever your holiday to you. Some wishes are a few days early, some a few days late, and some on time but you get the point. Go celebrate, enjoy food, family, and friends.
We are having a low key celebration our selves. Well several celebrations over the next few days. Lots of entertainment means lots of fun but lots of tired me, who might get cranky and live on pain meds. But we even have some lightly falling snow outside the window to admire.
But I will have fun. I will pretend I am on a mini medical vacation. I don't have any doctor appointments for another ten days. I will attempt to pretend I am healthy and enjoy the season. But I will still blog, cynically as usually.
Happy Holidays!
We are having a low key celebration our selves. Well several celebrations over the next few days. Lots of entertainment means lots of fun but lots of tired me, who might get cranky and live on pain meds. But we even have some lightly falling snow outside the window to admire.
But I will have fun. I will pretend I am on a mini medical vacation. I don't have any doctor appointments for another ten days. I will attempt to pretend I am healthy and enjoy the season. But I will still blog, cynically as usually.
Happy Holidays!
Monday, December 24, 2012
I have lots of optimistic reading to do today
I can't blog about these articles because:
A. Its too early in the day and my brain is not awake enough to absorb them.
B. I slept really badly last night and I am tired and crankiness may loom in my day.
C. They look long and complicated - a tad daunting, see A and B above.
But here are links to them:
Drug Aims to Make Several Types of Cancer Cells Self Destruct - http://www.nytimes.com/2012/12/23/health/new-drugs-aim-to-make-cells-destroy-cancer.html?ref=science&_r=1&
Is the Cure for Cancer Inside You? - http://www.nytimes.com/2012/12/23/magazine/is-the-cure-for-cancer-inside-you.html?pagewanted=1&_r=3&hp&
I promise to read them, digest them, and give you my opinion in the coming days.
I slept really badly because things hurt. Let me count the ways - back, hips, shoulder, elbow, feet, and hands. I don't think I left anything out but I might have. Oh yes, there was the overly friendly cat who kept on doing donuts on the bed over me. I think he was hungry. But he was annoying.
Its a good thing I have optimistic reading to do today because where does one's mind go when one is awake in the middle of the night? Down that DARK AND EVIL ROAD. You know the one. The one that asks things like:
- the pain isn't because of RA and fibro, its must be the return of the evil cancer cooties.
- when is my next doctor appointment, who is it with and what questions do I have to ask them?
- did I forget to get anyone's Christmas gift?
- and lastly why didn't I balance the check book since the mortgage is due later this week?
But I digress. I will optimistically read later today. First I need to finish waking up, go to the grocery store, and then to the gym. And take a nap.
PS the picture at the top of my blog is from our hotel room window at sunrise at Southport, ME in September.
A. Its too early in the day and my brain is not awake enough to absorb them.
B. I slept really badly last night and I am tired and crankiness may loom in my day.
C. They look long and complicated - a tad daunting, see A and B above.
But here are links to them:
Drug Aims to Make Several Types of Cancer Cells Self Destruct - http://www.nytimes.com/2012/12/23/health/new-drugs-aim-to-make-cells-destroy-cancer.html?ref=science&_r=1&
Is the Cure for Cancer Inside You? - http://www.nytimes.com/2012/12/23/magazine/is-the-cure-for-cancer-inside-you.html?pagewanted=1&_r=3&hp&
I promise to read them, digest them, and give you my opinion in the coming days.
I slept really badly because things hurt. Let me count the ways - back, hips, shoulder, elbow, feet, and hands. I don't think I left anything out but I might have. Oh yes, there was the overly friendly cat who kept on doing donuts on the bed over me. I think he was hungry. But he was annoying.
Its a good thing I have optimistic reading to do today because where does one's mind go when one is awake in the middle of the night? Down that DARK AND EVIL ROAD. You know the one. The one that asks things like:
- the pain isn't because of RA and fibro, its must be the return of the evil cancer cooties.
- when is my next doctor appointment, who is it with and what questions do I have to ask them?
- did I forget to get anyone's Christmas gift?
- and lastly why didn't I balance the check book since the mortgage is due later this week?
But I digress. I will optimistically read later today. First I need to finish waking up, go to the grocery store, and then to the gym. And take a nap.
PS the picture at the top of my blog is from our hotel room window at sunrise at Southport, ME in September.
Sunday, December 23, 2012
The femara dilemma
With breast cancer there is diagnosis, stress, depression, surgery, more stress, lymphedema worries, chemotherapy, baldness, neuropathy, weight gain, radiation, peeling skin, fatigue, stress, tamoxifen/aromatase inhibitors, slightly less stress, and through all of this is the ongoing care of your oncologists, surgeons, and other doctors.
I was diagnosed at the end of May 2007. I had surgery in both June and July. I started chemo on August 1 (some dates just stick in your brain) and finished chemo in mid December (where I bought myself an expensive watch as a gift), had a bad MRI and had more surgery (benign but stressful). January 2008 I began radiation and ended at the end of February. In about January sometime I was put on Tamoxifen for 2+ years. June 2010 I switched to Femara for another 2+ years. In September this year when I saw my oncologist she discussed going off Femara at my next visit to her which is next month.
As I filled up my weekly pill boxes I contemplated the fact that I don't have enough Femara tables to get me to my next appointment which is a paltry 15 days away. I have been going back and forth on this one. I know this is an emotional decision. There are no real benefits to taking Femara longer. But this is my last breast cancer treatment - that's it. No more. None. I just go to visits with doctors periodically where they will poke and pry and ask me how I feel (and look for potential rogue cancer cooties).
But emotionally am I ready to 'pull the plug' on all my treatment? I know this is why my medical oncologist brought this up when I met with her last fall. She wanted me to get prepared for this. At first I thought it was no big deal. But it is.
I have been waffling on this and caved in. This morning I placed a mail order to refill my Femara. It should arrive here just before I run out. Which will be a few days before my appointment. I would be happy to take fewer prescriptions but this is the last means of support against the evil cancer cooties.
I think at my appointment I will discuss my emotional attachment to Femara with my oncologist. My inner wimp is prevailing here at this point. Maybe I'll bring my refill with me and turn them over to her if I can't cut myself off.
I was diagnosed at the end of May 2007. I had surgery in both June and July. I started chemo on August 1 (some dates just stick in your brain) and finished chemo in mid December (where I bought myself an expensive watch as a gift), had a bad MRI and had more surgery (benign but stressful). January 2008 I began radiation and ended at the end of February. In about January sometime I was put on Tamoxifen for 2+ years. June 2010 I switched to Femara for another 2+ years. In September this year when I saw my oncologist she discussed going off Femara at my next visit to her which is next month.
As I filled up my weekly pill boxes I contemplated the fact that I don't have enough Femara tables to get me to my next appointment which is a paltry 15 days away. I have been going back and forth on this one. I know this is an emotional decision. There are no real benefits to taking Femara longer. But this is my last breast cancer treatment - that's it. No more. None. I just go to visits with doctors periodically where they will poke and pry and ask me how I feel (and look for potential rogue cancer cooties).
But emotionally am I ready to 'pull the plug' on all my treatment? I know this is why my medical oncologist brought this up when I met with her last fall. She wanted me to get prepared for this. At first I thought it was no big deal. But it is.
I have been waffling on this and caved in. This morning I placed a mail order to refill my Femara. It should arrive here just before I run out. Which will be a few days before my appointment. I would be happy to take fewer prescriptions but this is the last means of support against the evil cancer cooties.
I think at my appointment I will discuss my emotional attachment to Femara with my oncologist. My inner wimp is prevailing here at this point. Maybe I'll bring my refill with me and turn them over to her if I can't cut myself off.
Saturday, December 22, 2012
The unsung heroes of modern medicine
We need to take a minute to remember a few things about our medical care. We see our doctors and nurses but what about everyone else?
We often forget those in the background. This article made me remember them all. We shoudl take a moment to thank them all.
- If you go to the doctor for a routine appointment, there is a receptionist and nurse and a doctor at the minimum.
- If you are sent for blood work, there is also the lab tech who draws your blood but also the people in the lab who test your blood.
- If you get an x-ray, there is the person who takes the x-ray plus the radiologist who reads them. Plus there are the people who maintain the machines.
- If you go for chemo, there is a receptionist, a nurse to take your vitals and draw blood, a medical oncologist to review your blood counts and recommend chemo doses, the nurse who gives you the infusion, the pharmacist who got all your meds ready.
- If you go for radiation, there is a receptionist, a radiation tech who gives you the radiation, a radiologist who reads your latest CT scan, a nurse who checks in on your and your radiation oncologist who supervises your care.
- If you have an operation there is an anesthesiologist, several nurses, assistant surgeon, etc.
- If you come to the hospital in an ambulance, there will be some EMTs, trauma nurses, a social worker, maybe a respiratory therapist, and more.
- What about residents in training, hospitalists who manage your care why you are an in patient?
- Never mind everyone else at the hospital or medical center who make the food, clean the rooms, coordinate care, schedule procedures, (wake you up to take your vitals in the middle of the night), and more.
We often forget those in the background. This article made me remember them all. We shoudl take a moment to thank them all.
Friday, December 21, 2012
Stupid politicians
Today I am running late. Or rather just slow. Somehow it is already 930 am and I am just getting to my blog. Usually I start my day earlier and quicker. I think I have a new evil cold. My co-workers had an evil cold and I think they shared it with me.
But I digress. Today's topic is this looming fiscal cliff crap. I usually do not blog about politics or other stuff but this is getting ridiculous. We have a bunch of politicians who never learned to play nice together. Therefore they disagree. They do not even agree to disagree. Well sometimes they agree to disagree with the other party on principle not because of the issue.
We now have what we call a stand off again. At the expense of the average American again. I am sure it will come down to a last minute vote which the media hypes into a cliff hanger.
Who wants to bet we pay higher taxes the first few weeks in January and then get the money back somehow? And the millionaires some how get to keep all their money?
What a bunch of bozos in Washington these days. They only care about their party and its polarized positions and not about the good of the country.
But I digress. Today's topic is this looming fiscal cliff crap. I usually do not blog about politics or other stuff but this is getting ridiculous. We have a bunch of politicians who never learned to play nice together. Therefore they disagree. They do not even agree to disagree. Well sometimes they agree to disagree with the other party on principle not because of the issue.
We now have what we call a stand off again. At the expense of the average American again. I am sure it will come down to a last minute vote which the media hypes into a cliff hanger.
Who wants to bet we pay higher taxes the first few weeks in January and then get the money back somehow? And the millionaires some how get to keep all their money?
What a bunch of bozos in Washington these days. They only care about their party and its polarized positions and not about the good of the country.
Thursday, December 20, 2012
Dear Brooke Burke- Chavet:
I don't know you, nor do I follow Dancing with the Stars or any show you have been on, I do feel some sort of camaraderie since I have also had thyroid cancer. While I greatly enjoyed the article about you and the eight things one should know about thyroid cancer, you missed number 9 and possibly more.
Number 9 is that thyroid cancer requires a lifetime of vigilance because it can and does recur 30-40 years later. This is important to remember. While most cancers tend to recur relatively soon after treatment, thyroid cancer is slow and takes its time.
As a result, even though you have nice clean results now you will need to have regular ultrasounds, that will eventually go to once every five years at a minimum. And there will be those fun whole body scans too.
I do not mean to be the bearer of doom and gloom but this is a fact that you should discuss with your doctor.
Sincerely,
a 31 years out thyroid cancer patient.
Number 9 is that thyroid cancer requires a lifetime of vigilance because it can and does recur 30-40 years later. This is important to remember. While most cancers tend to recur relatively soon after treatment, thyroid cancer is slow and takes its time.
As a result, even though you have nice clean results now you will need to have regular ultrasounds, that will eventually go to once every five years at a minimum. And there will be those fun whole body scans too.
I do not mean to be the bearer of doom and gloom but this is a fact that you should discuss with your doctor.
Sincerely,
a 31 years out thyroid cancer patient.
Wednesday, December 19, 2012
Its a good thing my mother made me eat tofu
Not really because I hate tofu. But I digress.
I guess it is now important that my mother made me eat tofu because according to a study at Georgetown, women who start eating soy as an adult tend to develop treatment resistant breast cancer tumors. But those who eat soy as a child and then through adulthood are more likely to develop tumors which are very sensitive to treatment.
This means I have eaten my lifetime quota of soy and have no reason to eat any more. I dislike tofu with a passion and have a good excuse for never eating it again. I tried soy yogurt once and found it tastes like Elmer's glue (according to my childhood memories) and tried giving it away to my 'healthy' friends who told me they didn't like it either.
Other things I never have to eat again:
And I will never eat tofu again.
I guess it is now important that my mother made me eat tofu because according to a study at Georgetown, women who start eating soy as an adult tend to develop treatment resistant breast cancer tumors. But those who eat soy as a child and then through adulthood are more likely to develop tumors which are very sensitive to treatment.
This means I have eaten my lifetime quota of soy and have no reason to eat any more. I dislike tofu with a passion and have a good excuse for never eating it again. I tried soy yogurt once and found it tastes like Elmer's glue (according to my childhood memories) and tried giving it away to my 'healthy' friends who told me they didn't like it either.
Other things I never have to eat again:
- processed food which has soy added to make it healthy - this includes many of the weight loss programs which supplement their foods with soy.
- Tofu (I add this again as a reflection of its 'ick' factor)
And I will never eat tofu again.
Tuesday, December 18, 2012
Squish the life out of them
Of all the weird cancer treatments I have heard, this one takes the cake. Or crunch. Here it is:
Squish the malignant cells back into normal size and they revert back to normal breast cancer cells.
I am sure squish is the technical term here and you will only 'feel a pinch'.
This study was presented at the American Society for Cell Biology in San Francisco recently so it wasn't done by Dr Jekyll with Igor as an assistant in the dungeon basement of an Eastern European castle.
Before you channel a mammogram machine gone bad, its done at the cell level.
Venugopalan and collaborators grew malignant breast epithelial cells in a gelatin-like substance that had been injected into flexible silicone chambers. The flexible chambers allowed the researchers to apply a compressive force in the first stages of cell development.
Over time, the compressed malignant cells grew into more organized, healthy-looking acini that resembled normal structures, compared with malignant cells that were not compressed. The researchers used time-lapse microscopy over several days to show that early compression also induced coherent rotation in the malignant cells, a characteristic feature of normal development.
Notably, those cells stopped growing once the breast tissue structure was formed, even though the compressive force had been removed.
[Read more at: http://medicalxpress.com/news/2012-12-revert-breast-cancer-cells.html#jCp]
But I am sure you will still only 'feel a pinch'.
Squish the malignant cells back into normal size and they revert back to normal breast cancer cells.
I am sure squish is the technical term here and you will only 'feel a pinch'.
This study was presented at the American Society for Cell Biology in San Francisco recently so it wasn't done by Dr Jekyll with Igor as an assistant in the dungeon basement of an Eastern European castle.
Before you channel a mammogram machine gone bad, its done at the cell level.
Venugopalan and collaborators grew malignant breast epithelial cells in a gelatin-like substance that had been injected into flexible silicone chambers. The flexible chambers allowed the researchers to apply a compressive force in the first stages of cell development.
Over time, the compressed malignant cells grew into more organized, healthy-looking acini that resembled normal structures, compared with malignant cells that were not compressed. The researchers used time-lapse microscopy over several days to show that early compression also induced coherent rotation in the malignant cells, a characteristic feature of normal development.
Notably, those cells stopped growing once the breast tissue structure was formed, even though the compressive force had been removed.
[Read more at: http://medicalxpress.com/news/2012-12-revert-breast-cancer-cells.html#jCp]
But I am sure you will still only 'feel a pinch'.
Monday, December 17, 2012
My Attitude Needs an Adjustment
I have been thinking (which we all know is not a good thing) recently and wonder if I have turned into a 'poor me' person - the bane of all patients. The next step might be hypochondria - which we really do not need.
So my medical life has been in a downward spiral for some years now. Its now at the point where my doctors have said to me 'you have been through a lot'. Most of my ailments have been ones I have dealt with, tightened my belt and moved on. But this rheumatoid and fibromyalgia stuff seems to be getting to me more than other ailments.
I have met all my personal medical requirements:
Before her party started, we managed to have a few minutes to talk about it. She said it took two years to get a diagnosis because she also had Lyme disease when her RA started. But she now really feels fine.
I decided I am jealous that she is in control of her RA (and still weighs the same that she did in high school). But two years to get it under control? I'm not sure I'm up to that.
But I digress. As I drove home from her party with my husband, I started to think. We left somewhat early because I got tired and was in pain. My friend and her husband were all going strong. I wanted to go home and go to bed.
I spent most of Sunday being lazy because I didn't have the 'oomph' to do much. While being lazy, I decided my attitude needs some adjustment so I can have more fun in my life and be perky again.
So my medical life has been in a downward spiral for some years now. Its now at the point where my doctors have said to me 'you have been through a lot'. Most of my ailments have been ones I have dealt with, tightened my belt and moved on. But this rheumatoid and fibromyalgia stuff seems to be getting to me more than other ailments.
I have met all my personal medical requirements:
- I can't have an ailment that I can't spell or pronounce.
- I have a treatment plan (for RA so far but not yet for fibro as they need to treat one first and then the other so we can tell if its working or not but there is a plan afoot for fibro as well).
- I have educated myself on both and joined online support groups.
- I will attend a monthly local chronic pain group.
- I can joke about it.
Before her party started, we managed to have a few minutes to talk about it. She said it took two years to get a diagnosis because she also had Lyme disease when her RA started. But she now really feels fine.
I decided I am jealous that she is in control of her RA (and still weighs the same that she did in high school). But two years to get it under control? I'm not sure I'm up to that.
But I digress. As I drove home from her party with my husband, I started to think. We left somewhat early because I got tired and was in pain. My friend and her husband were all going strong. I wanted to go home and go to bed.
I spent most of Sunday being lazy because I didn't have the 'oomph' to do much. While being lazy, I decided my attitude needs some adjustment so I can have more fun in my life and be perky again.
Sunday, December 16, 2012
A picture paints 1000 words
We all hear 'we need to wait for the pathology report' and 'Tamoxifen prevents breast cancer recurrence'. But what exactly does this look like? I had no idea. Now I do, thanks to Cure Magazine (www.curetoday.com) - go get a subscription if you have or had cancer and don't receive it.

On the left we have: Estrogen binds to the estrogen receptor, initiating a cascade of events that activate certain genes leading to tumor cell growth.
On the right we have:Tamoxifen blocks estrogen binding to the estrogen receptor, stopping tumor growth.
 Starting from the left:
Starting from the left:
Immunohistochemitry (IHC) for the estrogen receptor in the cell nucleus. Left to right: Low, mildly positive, and highly positive.
Next image: Flourescence in situ hybridization (FISH) tests for Her2 expression by staining a control chromosome green and the Her2 receptor pink.
Final image: Immunohistochemistry (IHC) tests show the Her2 receptor at the cell surface.

On the left we have: Estrogen binds to the estrogen receptor, initiating a cascade of events that activate certain genes leading to tumor cell growth.
On the right we have:Tamoxifen blocks estrogen binding to the estrogen receptor, stopping tumor growth.

Immunohistochemitry (IHC) for the estrogen receptor in the cell nucleus. Left to right: Low, mildly positive, and highly positive.
Next image: Flourescence in situ hybridization (FISH) tests for Her2 expression by staining a control chromosome green and the Her2 receptor pink.
Final image: Immunohistochemistry (IHC) tests show the Her2 receptor at the cell surface.
Saturday, December 15, 2012
Hindsight is always 20/20
So now that you have been down the cancer road once, what have you learned? What would you do differently if there was a 'next time' (if you were so 'lucky')?
I am sure you are saying all sorts of things to yourself about how you would do more research, find more specialists, get a third opinion, make sure you dotted your "i's" and crossed your "t's" and had a bit more style while in chemo. There would be so many things you would do differently.
This man had cancer and then twenty years later thought he might have it again. He did learn from the first round but it was still traumatizing.
I can tell you at the second diagnosis, it is still just as shocking, upsetting, scary, and traumatizing as it was the first time. You might be slightly better prepared to act to your hindsight but you still have to get past that trauma.
I did make some resolutions - one that cancer wasn't going to suck the life out of me for a second time. I did start this little blog and I have been more proactive in my health care. But still I face the same fears and anxieties.
A few years after my breast cancer diagnosis my husband had a little brush with colorectal cancer. I remember sitting in the doctor's office with him. My husband had already been in the other chair where he was the caregiver there for support to take notes and ask questions but he was now the one receiving and digesting the information about his body. The doctor was trying to form into words what he needed to tell us about surgery, treatment, and options. I spoke up and said I have had cancer twice so we are already familiar with a lot of this. The doctor relaxed a little and started giving us information and options.
Without cancer twice, would I have spoken up? Probably not. I would have been the little blob in fear with all the stress. But I had learned to ask questions and not accept medical advice from only one source.
Hindsight is 20/20 and we can paper our walls with "woulda, shoulda, coulda's" but we hope we learn from our life experiences so we can have a better experience the next time.
I am sure you are saying all sorts of things to yourself about how you would do more research, find more specialists, get a third opinion, make sure you dotted your "i's" and crossed your "t's" and had a bit more style while in chemo. There would be so many things you would do differently.
This man had cancer and then twenty years later thought he might have it again. He did learn from the first round but it was still traumatizing.
I can tell you at the second diagnosis, it is still just as shocking, upsetting, scary, and traumatizing as it was the first time. You might be slightly better prepared to act to your hindsight but you still have to get past that trauma.
I did make some resolutions - one that cancer wasn't going to suck the life out of me for a second time. I did start this little blog and I have been more proactive in my health care. But still I face the same fears and anxieties.
A few years after my breast cancer diagnosis my husband had a little brush with colorectal cancer. I remember sitting in the doctor's office with him. My husband had already been in the other chair where he was the caregiver there for support to take notes and ask questions but he was now the one receiving and digesting the information about his body. The doctor was trying to form into words what he needed to tell us about surgery, treatment, and options. I spoke up and said I have had cancer twice so we are already familiar with a lot of this. The doctor relaxed a little and started giving us information and options.
Without cancer twice, would I have spoken up? Probably not. I would have been the little blob in fear with all the stress. But I had learned to ask questions and not accept medical advice from only one source.
Hindsight is 20/20 and we can paper our walls with "woulda, shoulda, coulda's" but we hope we learn from our life experiences so we can have a better experience the next time.
Friday, December 14, 2012
Life after cancer
There is a term for life after cancer. It is 'Survivorship'. I am not a fan of the word at all. I consider survivor a label and all I have ever survived is a bunch of doctor appointments. But I digress.
There is now focus on 'survivorship' studies or the lack of them. Doctors focus on treating patients but historically have been paying less attention to the patient's quality of life issues after treatment. It is not uncommon for cancer treatment to leave patients with a range of issues. This new field is also called 'patient activation' (which isn't much better than the 's-word'. It provides "education, resources, and services for issues of survivors such as sexuality, cognitive issues, fertility, neuropathy, returning back to primary care, depression and late effects such as second cancers and cardiac issues."
If you think about how harsh cancer treatment really is compounded by the emotions behind a diagnosis, it is not surprising that the patients are left with such a range issues.
It is just sad that it has taken modern medicine so long to realize that we do need help after treatment.
There is now focus on 'survivorship' studies or the lack of them. Doctors focus on treating patients but historically have been paying less attention to the patient's quality of life issues after treatment. It is not uncommon for cancer treatment to leave patients with a range of issues. This new field is also called 'patient activation' (which isn't much better than the 's-word'. It provides "education, resources, and services for issues of survivors such as sexuality, cognitive issues, fertility, neuropathy, returning back to primary care, depression and late effects such as second cancers and cardiac issues."
If you think about how harsh cancer treatment really is compounded by the emotions behind a diagnosis, it is not surprising that the patients are left with such a range issues.
It is just sad that it has taken modern medicine so long to realize that we do need help after treatment.
Thursday, December 13, 2012
A New Tool for Thyroid Cancer Diagnosis
Thyroid cancer has the fastest growing rate of incidence in the US of any cancers. The standard procedure to diagnose thyroid cancer is the doctor presses on the patients throat and asks them to swallow - this is to feel for any nodules or lumps. Other symptoms may appear such as a swallowing problems, a sore throat or speaking problems.
If a problem is suspected, the next usual step is an ultrasound to see if a determination can be made. 1/3 of all ultrasounds are inconclusive - meaning a determination can't be made to determine malignancy.
The next step is a thyroidectomy where the patient if benign will spend their life on synthetic thyroid hormone - which is not quite the real thing. The problem arises in that for those with inconclusive ultrasounds only 25% of them are diagnosed with cancer at their thryoidectomy. Or 75% have unneeded surgery.
But the new hero comes riding in in the form of a new gene test which has a 90% success rate for determining if thyroid cancer or not.
This means patients no longer have unneeded surgery which puts them into a life with out a thyroid which is fairly significant issue. And it reduces costs for for the patient and the medical care.
Okay some good progress for cynical me.
If a problem is suspected, the next usual step is an ultrasound to see if a determination can be made. 1/3 of all ultrasounds are inconclusive - meaning a determination can't be made to determine malignancy.
The next step is a thyroidectomy where the patient if benign will spend their life on synthetic thyroid hormone - which is not quite the real thing. The problem arises in that for those with inconclusive ultrasounds only 25% of them are diagnosed with cancer at their thryoidectomy. Or 75% have unneeded surgery.
But the new hero comes riding in in the form of a new gene test which has a 90% success rate for determining if thyroid cancer or not.
This means patients no longer have unneeded surgery which puts them into a life with out a thyroid which is fairly significant issue. And it reduces costs for for the patient and the medical care.
Okay some good progress for cynical me.
Wednesday, December 12, 2012
Stress is evil
So yesterday I had a bad day. It was compounded by stress. This was my day.
Today will not help. I have an 8am conference call to work on a client's database. At 9am a contractor is showing up to fix our basement door (so its no longer a burglar's dream). I also have to get out a mailing for work, work on our Christmas cards, and go to the grocery store. I was supposed to go out to dinner as well but I declined.
I think I am not coping well because I am tired, I get tired easily, and pain seems to be dominating my life which is living with fibromyagia. I need better ways to cope to reduce stress. Stress sucks. Maybe I need more naps.
- I went to work and needed to fix an iPad (and I've never used one before).
- I needed to fix two co-workers easy email issues.
- I needed to fix another co-workers very difficult email issue.
- At one point I stood up from my chair, tripped, caught myself on the next cubicle wall which gave me a jolt that hurt my hip and back and shoulder.
- I never got ANY of my work done.
- I left work and went to the gym where my hip and shoulder really hurt so I went home.
- I had cheese and crackers for dinner.
- I had a box of stuff that I bought on line ready to be taped up and returned with all the paperwork and my husband thought he was being helpful and unpacked the box, threw out the packing materials and paperwork.
- I went to a meeting which was full of dissent and disagreements.
- I came home and was VERY stressed out, not coping well with the stress at all.
Today will not help. I have an 8am conference call to work on a client's database. At 9am a contractor is showing up to fix our basement door (so its no longer a burglar's dream). I also have to get out a mailing for work, work on our Christmas cards, and go to the grocery store. I was supposed to go out to dinner as well but I declined.
I think I am not coping well because I am tired, I get tired easily, and pain seems to be dominating my life which is living with fibromyagia. I need better ways to cope to reduce stress. Stress sucks. Maybe I need more naps.
Tuesday, December 11, 2012
Five New Breast Cancer Controversies
At the San Antonio Breast Cancer Symposium last week, there are five new breast cancer discoveries controversies. I know a couple of people who was there and hope to hear more from them but this is what I have for opinions so far:
1. Claim: Chemobrain starts before starting chemotherapy.Results were presented to show that in a study women who had not gone through chemo were showing the symptoms - which can also be caused by worry and fatigue. Hello, if you are diagnosed with cancer, have surgery, and are facing chemotherapy perhaps you might be a tad bit worried and tired?
My take on this is that first of all this study was done by people who don't believe chemo brain is real. Symptoms of chemobrain could also be the same as those caused by worry and fatigue. But the difference with chemobrain is the symptoms do not go away once you stop stressing and get some rest. There is a difference.
2. Claim: Taking Tamoxifen for ten years is better than five years. First of all this isn't new. This is just a new study that they are showing results. My take is that more testing is needed as it goes against what has previously been shown.
3. Claim: Doubling the dose of fulvestrant is better. I have no opinion here as I do not know anything about this drug.
4. Claim: Twice as long is not better with Herceptin. My take is this is only confirming previous research.
5. Claim: Avastin isn't indicated for breast cancer. My take is this is not new. This has been resolved a while back.
Let me just say I am not a doctor or researcher, I am merely a patient. I admit I am not perfect so I could be wrong and these are my opinions.
So overall, We have one new claim that I, and many other women with chemobrain, disagree with completely. One claim I can't say anything about. And three claims is that I say are not new.
Hmmm.... I think I need some more proof to show that these are truly new and breakthroughs in some way. But I am not buying most of these.
1. Claim: Chemobrain starts before starting chemotherapy.Results were presented to show that in a study women who had not gone through chemo were showing the symptoms - which can also be caused by worry and fatigue. Hello, if you are diagnosed with cancer, have surgery, and are facing chemotherapy perhaps you might be a tad bit worried and tired?
My take on this is that first of all this study was done by people who don't believe chemo brain is real. Symptoms of chemobrain could also be the same as those caused by worry and fatigue. But the difference with chemobrain is the symptoms do not go away once you stop stressing and get some rest. There is a difference.
2. Claim: Taking Tamoxifen for ten years is better than five years. First of all this isn't new. This is just a new study that they are showing results. My take is that more testing is needed as it goes against what has previously been shown.
3. Claim: Doubling the dose of fulvestrant is better. I have no opinion here as I do not know anything about this drug.
4. Claim: Twice as long is not better with Herceptin. My take is this is only confirming previous research.
5. Claim: Avastin isn't indicated for breast cancer. My take is this is not new. This has been resolved a while back.
Let me just say I am not a doctor or researcher, I am merely a patient. I admit I am not perfect so I could be wrong and these are my opinions.
So overall, We have one new claim that I, and many other women with chemobrain, disagree with completely. One claim I can't say anything about. And three claims is that I say are not new.
Hmmm.... I think I need some more proof to show that these are truly new and breakthroughs in some way. But I am not buying most of these.
Monday, December 10, 2012
DNA mapping
Hmmm.... I like this concept of mapping the DNA of cancer patients. Actually the UK's National Health Service has announced a plan to map the DNA of 100,00 patients with rare diseases and cancers. (And the immediate comments on the article are how did the British government come up with the 100 million pounds to pay for this during the time of austerity.)
Politics and financing (and squabbling) aside I think this is a good idea. I have always wondered why I have been lucky enough to have cancer twice while the rest of my family remains healthy. If my DNA would tell something about it, I would welcome the opportunity to learn more about me.
Actually I would not be surprised if a lot of the secrets of us less than healthy people could be discovered in our DNA. Now that the price has dropped significantly to between 5 and 10 thousand pounds, it is getting within the range of affordability (come on, work with me if some cancer drugs can cost upwards of $100,000/year this is affordable). Maybe a little more money should be spent on looking at why some people seem to get the ailments. (I could be their poster child.) Instead of just throwing money at a cure.
An ounce of prevention is worth a pound of cure.
Politics and financing (and squabbling) aside I think this is a good idea. I have always wondered why I have been lucky enough to have cancer twice while the rest of my family remains healthy. If my DNA would tell something about it, I would welcome the opportunity to learn more about me.
Actually I would not be surprised if a lot of the secrets of us less than healthy people could be discovered in our DNA. Now that the price has dropped significantly to between 5 and 10 thousand pounds, it is getting within the range of affordability (come on, work with me if some cancer drugs can cost upwards of $100,000/year this is affordable). Maybe a little more money should be spent on looking at why some people seem to get the ailments. (I could be their poster child.) Instead of just throwing money at a cure.
An ounce of prevention is worth a pound of cure.
Sunday, December 9, 2012
Its a vast conspiracy

Tamoxifen has been known to cause endometrial cancer. Chemotherapy in general causes chemobrain and temporary or permanent neuropathy. Hormonal treatments cause weight gain. But you are supposed to stay thin to prevent increasing your risk of recurrence.
I can go on and on.
Its a vast conspiracy I tell you.
Saturday, December 8, 2012
Will I always compare fatigue now to cancer treatment fatigue?
Anyone who has gone through chemo can tell you about fatigue where you sit stupidly on the living sofa/arm chair staring blankly at a television screen not remembering a thing you watched. Fatigue where sleeping late turns into an afternoon nap. Being so tired you felt like you were hit by a truck upon waking up in the morning.
Last night I went to a craft fair where I had a table (anyone want to buy a hand knit or crocheted scarf?) that ended at 9pm which is VERY close to my bedtime these days. As I was driving home I thought I was really tired, like chemotherapy tired or end of radiation treatment tired. But I am not in chemo or finishing radiation, I am living the rheumatoid/fibromyalgia life where fatigue is part of the package. How fun (not really).
Then I started thinking again (I know I really shouldn't do this - think that is) and wondered am I forever going to compare my level of fatigue with how I felt during cancer treatment? I mean I used to think I was feeling exhausted and tired like I had skied hard, or climbed a relatively large mountain, or spent the day running around on the beach. Now I just compare it with chemo or radiation fatigue. Well grr.
I think my life needs a better perspective so I can skip thinking about chemo and radiation (I am sure that will be SO easy to do) and think being tired after something fun. And I'll have to take up napping and refine it to an art form.
Last night I went to a craft fair where I had a table (anyone want to buy a hand knit or crocheted scarf?) that ended at 9pm which is VERY close to my bedtime these days. As I was driving home I thought I was really tired, like chemotherapy tired or end of radiation treatment tired. But I am not in chemo or finishing radiation, I am living the rheumatoid/fibromyalgia life where fatigue is part of the package. How fun (not really).
Then I started thinking again (I know I really shouldn't do this - think that is) and wondered am I forever going to compare my level of fatigue with how I felt during cancer treatment? I mean I used to think I was feeling exhausted and tired like I had skied hard, or climbed a relatively large mountain, or spent the day running around on the beach. Now I just compare it with chemo or radiation fatigue. Well grr.
I think my life needs a better perspective so I can skip thinking about chemo and radiation (I am sure that will be SO easy to do) and think being tired after something fun. And I'll have to take up napping and refine it to an art form.
Friday, December 7, 2012
News flash: confusion among cancer patients
That's not really news. Nor is it the real title. This is the real one:
Thursday, December 6, 2012
Stop changing your mind. You are confusing (and scaring) the patients.
They keep changing their minds. These are the evil 'them' who are out to confuse all the patients they cant kill off. They just released a new study that breast cancer patients should have ten years of tamoxifen, and not five. I thought I was done with it. I was on tamoxifen for 2 years and am just finishing up on Femara for another three. I would be done in January. But will ask my oncologist if there is any reason to go back on Tamoxifen.
Truth be told, I would be perfectly happy to have one fewer daily medication to take and was starting to look forward to the end of Arimidex which is currently scheduled for January.
In an evil little psychotic way, I am glad to read that even the oncologists are confused by this. You can read on below but the gist of it is women who took tamoxifen for 10 years had a 12% rate of dying from breast cancer ove rthe 15 year study compared with at 15% risk for those who took a placebo after the first five years. Howevr about 3% of women who took tamoxifen developed endometrial cancer.
"“It’s going to be practice-changing, in my view, immediately for pre-menopausal women with breast cancer,” said Dr. Eric Winer, chief of women’s cancers at the Dana-Farber Cancer Institute who was attending the San Antonio cancer conference where the results were presented Wednesday. Those who have “estrogen-receptor positive” breast cancer, the type that responds to tamoxifen, will probably be advised to continue taking tamoxifen for an additional five years, he said.
Younger breast cancer patients who stopped taking tamoxifen years earlier may be counseled to start taking the drugs again.
On an individual level, breast cancer patients will need to weigh their tamoxifen options carefully.
On an individual level, however, breast cancer patients will
need to weigh their options carefully. Endometrial cancer is a real
concern, but it is usually more common in women over age 60. Patients
should also realize that “the benefit isn’t huge, it’s modest,” Winer
said.
Some women can’t tolerate tamoxifen and are eager to get off the drug as quickly as possible. They might have hot flashes, moodiness, and vaginal dryness making sex very painful. “About 10 to 15 percent of women don’t like being on it,” Winer added, “and unfortunately, younger women seem to have more of these side effects.”
Those with small, non-aggressive tumors with no spread to nearby lymph nodes might consider taking tamoxifen for only five years if they’re plagued by side effects since their risk of recurrence is very small. Those with larger, more aggressive tumors, however, might feel more compelled to stay on the drug for a decade.
For women whose breast cancer was diagnosed after menopause, the picture gets even more complicated. They’re usually given newer drugs called aromatase inhibitors (Arimidex, Femara, Aromasin) in addition to or instead of tamoxifen for a total of five years of treatment. Post-menopausal patients at Dana-Farber typically get two years of tamoxifen followed by five years of aromatase inhibitors.
“I’ve long believed that these extra years of treatment would help,” said Winer. That’s because with estrogen-receptor positive cancers, half of all recurrences happen beyond five years of diagnosis.
The new study found that 21 percent of those taking tamoxifen for 10 years had a recurrence during the study compared with 25 percent taking tamoxifen for the shorter period. The biggest differences in recurrence rates were seen between 10 and 15 years after the cancer diagnosis.
“That was confusing to some of the oncologists at the meeting,” Winer said, but it could have to do with tamoxifen’s cancer-preventing benefits lasting for up to five years after women stop taking the drug.
Post-menopausal breast cancer patients could be given the option to take estrogen-blocking drugs for longer, but oncologists might be left in a quandary about which drugs to give and for how long.
“Should these patients be given 10 years of treatment with an aromatase inhibitor? Should they have 5 years of an aromatase inhibitor followed by 5 years of tamoxifen? Would more than 10 years of tamoxifen be even better than 10 years? No data exist to support any of these options,” wrote Dr. Trevor Powles, an oncologist at the Cancer Centre
London in England, in an editorial that accompanied the study."
This article is full of all sorts of 'warm fuzzy' news. Did you notice the statistic about recurrence rates highest between 10-15 years after diagnosis? I'm overjoyed.
This may have been a long awaited study but all it did was confuse and scare the patients and make them all want to call their oncologist right away and ask what impact this has on their treatment.
Truth be told, I would be perfectly happy to have one fewer daily medication to take and was starting to look forward to the end of Arimidex which is currently scheduled for January.
In an evil little psychotic way, I am glad to read that even the oncologists are confused by this. You can read on below but the gist of it is women who took tamoxifen for 10 years had a 12% rate of dying from breast cancer ove rthe 15 year study compared with at 15% risk for those who took a placebo after the first five years. Howevr about 3% of women who took tamoxifen developed endometrial cancer.
"“It’s going to be practice-changing, in my view, immediately for pre-menopausal women with breast cancer,” said Dr. Eric Winer, chief of women’s cancers at the Dana-Farber Cancer Institute who was attending the San Antonio cancer conference where the results were presented Wednesday. Those who have “estrogen-receptor positive” breast cancer, the type that responds to tamoxifen, will probably be advised to continue taking tamoxifen for an additional five years, he said.
Younger breast cancer patients who stopped taking tamoxifen years earlier may be counseled to start taking the drugs again.
On an individual level, breast cancer patients will need to weigh their tamoxifen options carefully.
Some women can’t tolerate tamoxifen and are eager to get off the drug as quickly as possible. They might have hot flashes, moodiness, and vaginal dryness making sex very painful. “About 10 to 15 percent of women don’t like being on it,” Winer added, “and unfortunately, younger women seem to have more of these side effects.”
Those with small, non-aggressive tumors with no spread to nearby lymph nodes might consider taking tamoxifen for only five years if they’re plagued by side effects since their risk of recurrence is very small. Those with larger, more aggressive tumors, however, might feel more compelled to stay on the drug for a decade.
For women whose breast cancer was diagnosed after menopause, the picture gets even more complicated. They’re usually given newer drugs called aromatase inhibitors (Arimidex, Femara, Aromasin) in addition to or instead of tamoxifen for a total of five years of treatment. Post-menopausal patients at Dana-Farber typically get two years of tamoxifen followed by five years of aromatase inhibitors.
“I’ve long believed that these extra years of treatment would help,” said Winer. That’s because with estrogen-receptor positive cancers, half of all recurrences happen beyond five years of diagnosis.
The new study found that 21 percent of those taking tamoxifen for 10 years had a recurrence during the study compared with 25 percent taking tamoxifen for the shorter period. The biggest differences in recurrence rates were seen between 10 and 15 years after the cancer diagnosis.
“That was confusing to some of the oncologists at the meeting,” Winer said, but it could have to do with tamoxifen’s cancer-preventing benefits lasting for up to five years after women stop taking the drug.
Post-menopausal breast cancer patients could be given the option to take estrogen-blocking drugs for longer, but oncologists might be left in a quandary about which drugs to give and for how long.
“Should these patients be given 10 years of treatment with an aromatase inhibitor? Should they have 5 years of an aromatase inhibitor followed by 5 years of tamoxifen? Would more than 10 years of tamoxifen be even better than 10 years? No data exist to support any of these options,” wrote Dr. Trevor Powles, an oncologist at the Cancer Centre
London in England, in an editorial that accompanied the study."
This article is full of all sorts of 'warm fuzzy' news. Did you notice the statistic about recurrence rates highest between 10-15 years after diagnosis? I'm overjoyed.
This may have been a long awaited study but all it did was confuse and scare the patients and make them all want to call their oncologist right away and ask what impact this has on their treatment.
Wednesday, December 5, 2012
Dating and cancer
There is nothing like a cancer diagnosis to kill off your dating life. I am happily married and have been for more than 7 years. Before that I was in the dating world for my entire 20s and 30s. I had thyroid cancer in 1981 and met my husband in 2002 so that in the intervening twenty years I was out in the dating world a fair amount. I did have one long term relationship, 7+ years, but I did have many romantic and not so romantic evenings. (I think if you have had cancer, you should be able to get a pass on all bad dates, especially bad blind dates!)
I was reading this article about "Dating with Cancer" and I started thinking. (I apologize in advance for allowing myself to think but sometimes I even have deep thoughts!) I had cancer and was treated over a summer and returned to college for my sophomore year. I think it was fairly common knowledge on the small campus (1000 students) that I had cancer over the summer.
I quickly learned not to start conversations on 'what I did on my summer vacation' with 'I had cancer' but sometimes my friends and I would talk about it. In terms of dating and intimacy, and when to talk about cancer, I think the right time to bring it up is when you feel comfortable with it. There is no right or wrong time to bring it up - once you are past the first few dates.
If you show up on your first date and they ask you to tell a few things about yourself and you start with 'I just finished chemotherapy for my 'fill in the blank' cancer, and go back to my oncologist next week to see what my latest PET scan said', you shoudln't be surprised if suddenly they develop a stomach virus and have to go home.
If you and your partner have a great and open relationship and can talk about everything, you may feel comfortable bringing it up casually.
If you are a badge wearing, card carrying member of the cancer club, and make it your life motto, you may find you need to find a badge wearer to be comfortable at your side.
If you consider your cancer to be part of you that takes you to the doctor more frequently than your friends, you are probably more relaxed about it and less stressed.
A few things I did learn over the years:
I will sum up my advice on dating and cancer with 'go with your gut'. If you meet a great new potential partner and start talking as much as you can, spending every second you can together. As your conversations unfold and get more and more personal, you start to reveal more about yourself.
When to bring it up? Maybe take a moment, pour a cup of coffee and sit down and say you have something important you want to tell them. Make it clear you aren't going to drop dead anytime soon and be factual and keep it light. Your partner may have questions then or wait to ask questions until later. If you keep it an open topic that can be discussed again in the future.
If your potential partner runs for the hills at the news you aren't in perfect health, its probably just as well you found out sooner.
I was reading this article about "Dating with Cancer" and I started thinking. (I apologize in advance for allowing myself to think but sometimes I even have deep thoughts!) I had cancer and was treated over a summer and returned to college for my sophomore year. I think it was fairly common knowledge on the small campus (1000 students) that I had cancer over the summer.
I quickly learned not to start conversations on 'what I did on my summer vacation' with 'I had cancer' but sometimes my friends and I would talk about it. In terms of dating and intimacy, and when to talk about cancer, I think the right time to bring it up is when you feel comfortable with it. There is no right or wrong time to bring it up - once you are past the first few dates.
If you show up on your first date and they ask you to tell a few things about yourself and you start with 'I just finished chemotherapy for my 'fill in the blank' cancer, and go back to my oncologist next week to see what my latest PET scan said', you shoudln't be surprised if suddenly they develop a stomach virus and have to go home.
If you and your partner have a great and open relationship and can talk about everything, you may feel comfortable bringing it up casually.
If you are a badge wearing, card carrying member of the cancer club, and make it your life motto, you may find you need to find a badge wearer to be comfortable at your side.
If you consider your cancer to be part of you that takes you to the doctor more frequently than your friends, you are probably more relaxed about it and less stressed.
A few things I did learn over the years:
- Never lie about your health to a partner. If you do not feel comfortable enough with them to tell them about your health honestly, they are not probably a good partner for you. Honesty is important in a relationship. And a surgical scar will always look like a surgical scar unless you put a tattoo over it to hide it.
- There is no line in the sand which says you must tell someone your medical history before sex. You do need to talk about STDS and birth control and all that stuff but you don't need to tell them about chemotherapy and recurrence rates.
- You really should have a full disclosure on your health before marriage as it would be unfair to your partner not to tell them the truth.
I will sum up my advice on dating and cancer with 'go with your gut'. If you meet a great new potential partner and start talking as much as you can, spending every second you can together. As your conversations unfold and get more and more personal, you start to reveal more about yourself.
When to bring it up? Maybe take a moment, pour a cup of coffee and sit down and say you have something important you want to tell them. Make it clear you aren't going to drop dead anytime soon and be factual and keep it light. Your partner may have questions then or wait to ask questions until later. If you keep it an open topic that can be discussed again in the future.
If your potential partner runs for the hills at the news you aren't in perfect health, its probably just as well you found out sooner.
Tuesday, December 4, 2012
Did having cancer change you?
They did a new study (because these pesky researchers need to stay employed) on how people who had been diagnosed with and treated for cancer were doing both physically and medically after treatment.
Well its about time. What did they think that after our oncologists and surgeons send us on our merry way and only want to see us yearly instead of weekly we would just be fine? Seriously. For patients, it has always been a cliff where treatment ends and we are supposed to cope just fine as we switch from constant monitoring to yearly check ups. The doctors abruptly cut the cord. Many patients have an emotional upheaval that coincides with this transition and seek additional support. Its nice that the medical field is taking a closer look at how we cope in the ensuing years.
The study looked at, from the patient's perspective, physical functioning, pain, fatigue, and depression. They compared them to normal people who had never been diagnosed with cancer and found that:
As we are aware I am not a doctor, researcher or anyone qualified in anyway shape or form to do research as I a merely a cancer person. BUT, as I look at the different cancers they list and the outcome issues, I had a few comments (of course);
Keep researching this one. There are lots of us who would be happy to help in the research.
Well its about time. What did they think that after our oncologists and surgeons send us on our merry way and only want to see us yearly instead of weekly we would just be fine? Seriously. For patients, it has always been a cliff where treatment ends and we are supposed to cope just fine as we switch from constant monitoring to yearly check ups. The doctors abruptly cut the cord. Many patients have an emotional upheaval that coincides with this transition and seek additional support. Its nice that the medical field is taking a closer look at how we cope in the ensuing years.
The study looked at, from the patient's perspective, physical functioning, pain, fatigue, and depression. They compared them to normal people who had never been diagnosed with cancer and found that:
- People who had breast, prostate or melanomas had the same or better quality of life as the people who had never had cancer.
- People who had cervical, blood, or colorectal cancers and cancers with a 5 year survival rate of less than 25% (liver, pancreas, and lung) had worse physical health related quality of life.
- People with cervical cancer and cancers with low survival rates had worse mental quality of life. The goal is to check again in five years and see how these groups are doing with the advances in treatment.
As we are aware I am not a doctor, researcher or anyone qualified in anyway shape or form to do research as I a merely a cancer person. BUT, as I look at the different cancers they list and the outcome issues, I had a few comments (of course);
- The people who did well were the ones who had the 'high visibility' cancers - breast, prostate, and melanoma. I think of these as high visibility as they get a lot of press. We have pinkificiation for breast cancer. We have PSA tests and possible over diagnosis of prostate cancer and its all over the media. Melanoma is ingrained in all of us as we use sunscreen since birth nowadays. These cancers are talked about, videoed, profiled, and media hyped to no end.
- The people who did poorly physically had the cancers that either had low survival rates or less popular/lower profile cancers. Are they less acceptable cancers to get? Are their treatment protocols more 'damaging' to the human body?
- The people who did poorly mentally had cancers with lower survival rates. This is the most logical to me. If you are told you have cancer and have a low chance of living more than a few years, what is your mental state going to be?
Keep researching this one. There are lots of us who would be happy to help in the research.
Monday, December 3, 2012
Changing through cancer

[Note this is some what of a girly topic so go away if you might be offended.] Yesterday I got together with some old friends. Meaning people I have know for 25-30 years. They were talking about menopause issues - hot flashes, weight gain, etc. They are all coping with the symptoms naturally. If only I was in the same boat as them. I opted not to speak up as my medical history makes me very different. They were complaining about the past year or two.
It made me realize how my medical issues have changed me. I had a hysterectomy due to fibroids in 2005. It left me with one ovary. Chemotherapy made that ovary inactive so I had the luxury of going through chemopause which takes care of any remaining chance to go through menopause naturally. Then you add the wonderful cancer hormonal treatments that add hot flashes, weight gain, and all sorts of other fun things to the mix, chemically as opposed to naturally. And its been more than five years....
One friend pulled out a book on coping with menopause that had been recommended to her. There was a chapter on the thyroid and what it controls and how it can change as you age. I can skip that chapter as I don't have one and haven't for decades. Most of the other chapters talked about how your body changes and how you can cope with the changes. Mine menopause was forced and dragging on and on.
As I was leaving one friend said 'I hope your back gets better'. That left me feeling that they really do not understand me. One, my back will not get better and I have been repeating this for years, and two, my back is not my primary generator of pain these days. I had brought up the fact that I have both RA and fibro earlier in the day but evidently it did not connect as being limitations that I cope with on a daily basis now.
Driving home I started thinking (which is particularly dangerous in the realm of multitasking to think and drive). These are my friends who I have known for decades. None of them read my blog, two of them are on Facebook and update about every few months, they infrequently email as well. These are my primary means of communication these days. So if they do not participate, we are not connecting very frequently at all.
We get together five times a year for our birthdays. We also get together in different sub groups at different times but I can go for weeks and months without communicating. A good part of it is me. It is more and more difficult for me to be able to get out and do things as much as I used to. This is not due to cancer but due to my back, RA, and fibro.
But how much did my cancers change me, particularly breast cancer due to its recency? I have significantly less tolerance for idiots, late people, and foolish wastes of time. My health is front and center in my life. Without cancer, would I be coping differently? I hope so.
Sunday, December 2, 2012
How to be a (un)healthy person
As I used to be a healthy person but can probably safely say I am no longer a healthy person, I must be highly skilled at being an (un)healthy person.
Tomorrow I really want to sleep in as I am working from home. I hope to make it to the gym or for a walk with a friend.
The life of an (un)healthy person requires lots of rest and medication. I will keep practicing.
- I can easily put myself in pain by doing basic things - bending over, stretching, moving the cat, looking for things, picking up my laptop. I no longer rush to get to the phone because it can be painful (the rushing part).
- My bedside table collection of medications and supplements has been relocated to my closet shelf - as it has outgrown its original space. And is still growing.
- I carefully plan my activities to try to limit pain levels. My husband recommends on activity per day and I am reluctant to admit he might be right. Yesterday I attempted two activities and spent three hours in bed after the first one so I never made it to the second.
- Doctor appointments and phone calls get first priority in the scheduling of my life.
- Those little grocery carts everywhere. I can't push around traditional grocery store carts because they make my back hurt. I cant carry a basket of stuff because of lymphedema and hand, elbow issues. I need a little cart or my husband to come with me if I can get more than a couple items.
- Special working hours so I can sleep in at least one morning a week. I cant get up more than a few days in a row with the alarm. I get really tired and need to sleep in - at least until 730 - a few days a week. Last week I had to get up six days in a row and was really dragging.
- Cooking lessons for my husband. He cooks better and better these days because he has been getting plenty of opportunities to practice. He is pretty good and just needs encouragement for the nights I am simply too tired.
Tomorrow I really want to sleep in as I am working from home. I hope to make it to the gym or for a walk with a friend.
The life of an (un)healthy person requires lots of rest and medication. I will keep practicing.
Saturday, December 1, 2012
Patenting Genes Again
I have blogged about this before here and here. Who owns our genes? According to Myriad Genetics, which 'owns' the BRCA genes and tests and gets to charge $3,000 per test, they own the two BRCA genes. That sounds stupid, doesn't it? Apparently Myriad Genetics is full of rocket scientists who believe they can own parts of the human body that naturally occur. Maybe we can start selling patent rights to our big toes or something to pay our medical bills.
Well stupidity now faces the US Justice system as the Supreme Court announced on 11/30/2012 that they will hear the case on whether companies can patent human genes. As science and medical research grows and focus more and more on genetics this ruling could affect medical research in decades to come.
The two sides come down to this:
"The justices' decision will likely resolve an ongoing battle between scientists who believe that genes carrying the secrets of life should not be exploited for commercial gain and companies that argue that a patent is a reward for years of expensive research that moves science forward."
If we take this a step farther could lawn seed companies claim they own the genes in the grass seed they breed to make greener lawns so that we would need to pay rent to walk barefoot on the grass? Or someone could patent oxygen and we could start paying rent to breathe.
I am sure that the people with the BRCA gene would be happy to get rid of it so if Myriad wants to own the gene, why can't people get paid to have it taken out of their body?
I am in favor of the scientists, patients, medical research, and good health. I am against corporate greed.
I mean, seriously? Get over it. But now since it is going to the Supreme Court I am sure your lawyers will be rich by the time a decision is reached.
Well stupidity now faces the US Justice system as the Supreme Court announced on 11/30/2012 that they will hear the case on whether companies can patent human genes. As science and medical research grows and focus more and more on genetics this ruling could affect medical research in decades to come.
The two sides come down to this:
"The justices' decision will likely resolve an ongoing battle between scientists who believe that genes carrying the secrets of life should not be exploited for commercial gain and companies that argue that a patent is a reward for years of expensive research that moves science forward."
If we take this a step farther could lawn seed companies claim they own the genes in the grass seed they breed to make greener lawns so that we would need to pay rent to walk barefoot on the grass? Or someone could patent oxygen and we could start paying rent to breathe.
I am sure that the people with the BRCA gene would be happy to get rid of it so if Myriad wants to own the gene, why can't people get paid to have it taken out of their body?
I am in favor of the scientists, patients, medical research, and good health. I am against corporate greed.
I mean, seriously? Get over it. But now since it is going to the Supreme Court I am sure your lawyers will be rich by the time a decision is reached.
Friday, November 30, 2012
Humor and cancer

I know Lorri who lost a leg to cancer and does a stand up routine about the shark.... Because its funnier than cancer.
I know lots of women with breast cancer who have a group on Facebook called 'Humor is the best medicine' and are always looking for the bright side of things.
This morning a Google alert brought me a link to a Huffington Post Blog about a new cartoonist, Kate Matthews, who has just published "The Little Pink Book of (Mostly) Cancer Cartoons (In Color)!". So of course I had to do some research (even though its early in the day) and found some more info on her, including the fact that she is working on a second book.
Here are some of my first favorites. I am sure I will find more...




If you aren't laughing or at least smiling, you might need to think about therapy.
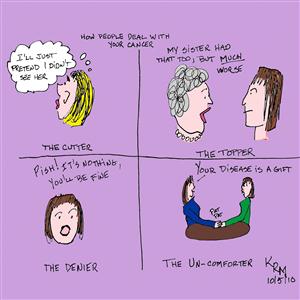{kind=link}
Thursday, November 29, 2012
Exercise and me
As an adult, I have been good at exercise. When I was a child, I was a dedicated athlete and ice skated daily before school, after school, on weekends, in skating shows, and basically a lot. Then I discovered being a teenager is more fun than spending your life at a skating rink and I was less of an athlete but generally active.
Eventually I discovered the benefit of a daily walk and walked my way through cancer, multiple surgeries (benign and malignant), and all sorts of fun. When I turned40 37 for the fourth time, I joined a gym. Then my back started to hurt and nearly a decade later, I joined a gym for decrepit people. They are familiar with decrepit people and health issues. In fact yesterday when I was there, there were two people on cardio machines while on oxygen.
As part of my expensive (but worth every penny) gym membership, I get a three month evaluation free of charge. Yesterday we talked about how I can exercise with RA and fibro to my best benefit. We went from the 'lets do lots of things to keep in as best shape as we can' to 'lets do a few things to preserve balance, flexibility, and strength without injury or causing more pain'.
Now my work out consists of 45-50 minutes of cardio instead of 40 and maybe 10 exercises at lower weights for 1 set of 25 reps instead of 20 exercises at medium weights for 2 sets of 15 reps.
I tried it yesterday. Last night I was hobbling around. Today I am still hobbling but haven't decided if it is caused by my workout yesterday. Today I am not exercising unless going to the grocery store counts. Pushing around a big grocery card can cause pain. I just won't buy a lot of heavy things.
I will get exercise again tomorrow I think. I have to skip a day between work outs or I end up in bed for a few days. Call me wimpy but call me alive.
Eventually I discovered the benefit of a daily walk and walked my way through cancer, multiple surgeries (benign and malignant), and all sorts of fun. When I turned
As part of my expensive (but worth every penny) gym membership, I get a three month evaluation free of charge. Yesterday we talked about how I can exercise with RA and fibro to my best benefit. We went from the 'lets do lots of things to keep in as best shape as we can' to 'lets do a few things to preserve balance, flexibility, and strength without injury or causing more pain'.
Now my work out consists of 45-50 minutes of cardio instead of 40 and maybe 10 exercises at lower weights for 1 set of 25 reps instead of 20 exercises at medium weights for 2 sets of 15 reps.
I tried it yesterday. Last night I was hobbling around. Today I am still hobbling but haven't decided if it is caused by my workout yesterday. Today I am not exercising unless going to the grocery store counts. Pushing around a big grocery card can cause pain. I just won't buy a lot of heavy things.
I will get exercise again tomorrow I think. I have to skip a day between work outs or I end up in bed for a few days. Call me wimpy but call me alive.
Wednesday, November 28, 2012
Coping, cooperating, and crankiness
I have had enough of serious blog posts on financial stuff and now am back to my normal (whatever that may be) level of zaniness in the crazy world of my health.
Monday I had a regular six month check up with the dentist. Something I hate/fear/detest more than almost anything - its right up there with those little medical adventures that might make me feel a 'twinge'. At the appointment, it was decided that I need two bonds which are relatively painless and quick and could help prevent future issues. I am all about my long term health (or what is left of it) so opted to have them. It was also pointed out that I have two older fillings on a single tooth which are stressing the tooth and cause it to start to crack. It was also decided it was in my best interest for what's left of my long term health to have them removed and replaced with a new white filling. Lo and behold, the dentist actually had a cancellation for yesterday morning at 830. I rearranged my schedule for yesterday morning and went for the appointment.
That was one of the worst dental appointments I have had in decades. First, I needed Novocaine on the top right and top left front, as well as the middle top right. Novocaine went in and the dentist got called away to check on another patient. The assisting tech decided to be proactive and put the clamp on my tooth to get ready for the rubber dam. Well that hurt/was uncomfortable/made me cringe and my stomach hurt. Not a good start. She took it off and tried a second one. The dentist returned and said to wait until the last minute. That's okay I was stressed already.
Then the old fillings took forever to drill off. Even the dentist said it did. She started explaining in detail that I didn't need. When she was done drilling, then she started putting in little wedges to rebuild my tooth and held it all in place with another clamp. She then moved on to the bonds but the drilling fun had taken so long I needed more novocaine. Then I went to work, with a stressed out stomach, feeling like I had a frozen face. When I got to work, I was told I didn't look very good.
That was on top of the continuing fight to get my new (old) pain patches for my RA/fibro. I was on the 5mcg pain patches but my doctor thought I should increase my dose to 10mcg because of my pain levels. The 5mcg ones I got from the mail order pharmacy for 3 months at a time with a paltry co-pay of $95. My doctor sent in a new prescription for the 10 mcg which showed up in a one month increment for the same paltry co-pay. I called the mail order pharmacy and was told they needed a new 90 day prescription. Then I called my doctors office and asked them to change the prescription to a 90 day supply.
Then I had an allergic reaction to thedamn pain patches. When I took off the patch, I had a perfect rectangle of rash which lined up exactly with the patch's adhesive. I called my doctors office again and asked them what were my options and was told to either try going with out the patches (which doesn't work unless I want to live on pain pills) or putting cortisone cream on my skin ahead of time to prevent the reaction.
I waited for thedamn rash to go away and tried again with the cortisone lotion. So far its working. Then another prescription showed up in the mail with its paltry $95 co-pay for one month of patches. And a note that said state law prevents them from sending more than 30 days at a time. I called the pharmacy again and was told it was by law but they weren't sure if why I had received 90 day supply of the 5mcg patches. I called my doctor's office again and asked for the 5mcg dose in a 90 day supply. Then I received another email saying a new prescription had been processed and will be sent to me. All I know is that it will have a $95 co-pay (that would be #3 this month) but I hope its for 3 months of the right patches that won't give me a rash.
In the meantime, back at the ranch so to speak, I have been coping with increasing pain, fatigue - where getting into my pjs at 7 pm sounds like a good idea, and trying to live a 'normal' life.
All this has led to some crankiness. And with my new RA meds, I have had to give up alcohol so I can't even have a glass of wine to cope. Crankiness is ensuing because the scale has not cooperated in making me a skinny alcohol free pain patient.
Monday I had a regular six month check up with the dentist. Something I hate/fear/detest more than almost anything - its right up there with those little medical adventures that might make me feel a 'twinge'. At the appointment, it was decided that I need two bonds which are relatively painless and quick and could help prevent future issues. I am all about my long term health (or what is left of it) so opted to have them. It was also pointed out that I have two older fillings on a single tooth which are stressing the tooth and cause it to start to crack. It was also decided it was in my best interest for what's left of my long term health to have them removed and replaced with a new white filling. Lo and behold, the dentist actually had a cancellation for yesterday morning at 830. I rearranged my schedule for yesterday morning and went for the appointment.
That was one of the worst dental appointments I have had in decades. First, I needed Novocaine on the top right and top left front, as well as the middle top right. Novocaine went in and the dentist got called away to check on another patient. The assisting tech decided to be proactive and put the clamp on my tooth to get ready for the rubber dam. Well that hurt/was uncomfortable/made me cringe and my stomach hurt. Not a good start. She took it off and tried a second one. The dentist returned and said to wait until the last minute. That's okay I was stressed already.
Then the old fillings took forever to drill off. Even the dentist said it did. She started explaining in detail that I didn't need. When she was done drilling, then she started putting in little wedges to rebuild my tooth and held it all in place with another clamp. She then moved on to the bonds but the drilling fun had taken so long I needed more novocaine. Then I went to work, with a stressed out stomach, feeling like I had a frozen face. When I got to work, I was told I didn't look very good.
That was on top of the continuing fight to get my new (old) pain patches for my RA/fibro. I was on the 5mcg pain patches but my doctor thought I should increase my dose to 10mcg because of my pain levels. The 5mcg ones I got from the mail order pharmacy for 3 months at a time with a paltry co-pay of $95. My doctor sent in a new prescription for the 10 mcg which showed up in a one month increment for the same paltry co-pay. I called the mail order pharmacy and was told they needed a new 90 day prescription. Then I called my doctors office and asked them to change the prescription to a 90 day supply.
Then I had an allergic reaction to the
I waited for the
In the meantime, back at the ranch so to speak, I have been coping with increasing pain, fatigue - where getting into my pjs at 7 pm sounds like a good idea, and trying to live a 'normal' life.
All this has led to some crankiness. And with my new RA meds, I have had to give up alcohol so I can't even have a glass of wine to cope. Crankiness is ensuing because the scale has not cooperated in making me a skinny alcohol free pain patient.
Tuesday, November 27, 2012
The Cost of Cancer Care, Part 4 - Waste
I am continuing my series on the costs of cancer I wanted to write about medical waste. But let's back up a minute, why am I pretending I am scholarly and writing about these 'big' topics in my little tiny blog? Because I think they are important. The medical costs a cancer patient incurs are amazingly high compared to other ailments - particularly in the first year after diagnosis and the last year of their life.
Cancer is becoming more treatable but is also becoming more expensive at alarming rates. The idea that a single chemotherapy infusion can cost over $10,000 is crazy. And unfortunately it is common place. Then if you take the infusion style chemo out of the hospital it becomes a pill that is covered by the pharmacy benefit which means it can costs hundreds of dollars per daily pill. So it may be physically easier on the patient to take a pill instead of receiving an infusion but is much more damaging on their wallet.
But I digress. Today I am writing about the broader spectrum of all medical costs. When I think of medical waste, I think of these big sterilized packages which are used to protect an IV kit and what isn't used is dumped in the trash. All those individually sterilized and sealed items where wrappers larger than the tool are thrown in the trash. By health standards, if a package is unsealed, anything that is not used is no longer sterile and goes in the trash. There are lots of single use items which make their way to the incinerators and landfills.
Unfortunately medical waste is also defined as a much larger problem. Medical waste often happens when there is a patchwork of care.
"Manhattan in New York City is a good example. Because healthcare utilization there is among the nation’s highest, Manhattan is seen as wasteful and inefficient. But it is a patch-quilt of wealth and poverty. Utilization in the low-income Bowery is double the rate of the affluent Upper East Side and Upper West Side, and utilization in Harlem, the poorest area, is more than triple (unpublished data). Without either, Manhattan’s utilization is among the lowest in the nation, lower even than Grand Junction, Colorado, whose healthcare system was held out by President Obama as a model for the nation. But like Grand Junction, the Upper East Side and Upper West Side of Manhattan have few African Americans and no poverty ghettos.
How much does the extra care in poor neighborhoods add to overall utilization costs within a region? The best estimate is 20% to 25%.[17] Yet, tragically, this fact is ignored—indeed, denied. For example, Dartmouth researchers mock the fact that “some physicians believe their hospitals or regions spend more because their patients are sicker and poorer” and declare, “regional differences in poverty explain almost none of the variation.”[19] In a similar manner, Nicholas Kristof, a columnist for The New York Times and an advocate for the poor globally, labeled as “opponents of health care reform” those who attributed poor outcomes to “America’s large underclass.”[20] In fact, poverty explains virtually all of the regional differences in utilization, and “America’s large underclass” accounts for virtually all of the differences in outcomes between the US and other nations.
Real healthcare reform would address these socioeconomic realities. Instead, the US is waging a regulatory “war” on exaggerated measures of waste, one that shows little promise of reducing costs or increasing quality but will assuredly crush “needed innovation by practicing physicians, who best understand the delivery of care.”[1] Moreover, because there are no risk adjusters for poverty, physicians whose low-income patients fail to meet federal utilization and quality norms will suffer financially, and hospitals whose poor patients have high readmission rates will be penalized. All the while, the “war on waste” will distract policymakers from building the social infrastructure that could lower the high healthcare costs of poverty. These are no ordinary times. For the first time, physicians and their patients are caught in the crosshairs of the “war on waste.”'
So where does this all leave us? The Republicans believe that market forces will help reduce costs and waste while the Democrats look for answers in the Affordable Care Act. What this tells me is that the system is flawed and needs changes which is nothing new. We can't look to politicians for reform as our sole solution. We need to look at the health care system to resolve this.
Cancer is becoming more treatable but is also becoming more expensive at alarming rates. The idea that a single chemotherapy infusion can cost over $10,000 is crazy. And unfortunately it is common place. Then if you take the infusion style chemo out of the hospital it becomes a pill that is covered by the pharmacy benefit which means it can costs hundreds of dollars per daily pill. So it may be physically easier on the patient to take a pill instead of receiving an infusion but is much more damaging on their wallet.
But I digress. Today I am writing about the broader spectrum of all medical costs. When I think of medical waste, I think of these big sterilized packages which are used to protect an IV kit and what isn't used is dumped in the trash. All those individually sterilized and sealed items where wrappers larger than the tool are thrown in the trash. By health standards, if a package is unsealed, anything that is not used is no longer sterile and goes in the trash. There are lots of single use items which make their way to the incinerators and landfills.
Unfortunately medical waste is also defined as a much larger problem. Medical waste often happens when there is a patchwork of care.
"Manhattan in New York City is a good example. Because healthcare utilization there is among the nation’s highest, Manhattan is seen as wasteful and inefficient. But it is a patch-quilt of wealth and poverty. Utilization in the low-income Bowery is double the rate of the affluent Upper East Side and Upper West Side, and utilization in Harlem, the poorest area, is more than triple (unpublished data). Without either, Manhattan’s utilization is among the lowest in the nation, lower even than Grand Junction, Colorado, whose healthcare system was held out by President Obama as a model for the nation. But like Grand Junction, the Upper East Side and Upper West Side of Manhattan have few African Americans and no poverty ghettos.
How much does the extra care in poor neighborhoods add to overall utilization costs within a region? The best estimate is 20% to 25%.[17] Yet, tragically, this fact is ignored—indeed, denied. For example, Dartmouth researchers mock the fact that “some physicians believe their hospitals or regions spend more because their patients are sicker and poorer” and declare, “regional differences in poverty explain almost none of the variation.”[19] In a similar manner, Nicholas Kristof, a columnist for The New York Times and an advocate for the poor globally, labeled as “opponents of health care reform” those who attributed poor outcomes to “America’s large underclass.”[20] In fact, poverty explains virtually all of the regional differences in utilization, and “America’s large underclass” accounts for virtually all of the differences in outcomes between the US and other nations.
Real healthcare reform would address these socioeconomic realities. Instead, the US is waging a regulatory “war” on exaggerated measures of waste, one that shows little promise of reducing costs or increasing quality but will assuredly crush “needed innovation by practicing physicians, who best understand the delivery of care.”[1] Moreover, because there are no risk adjusters for poverty, physicians whose low-income patients fail to meet federal utilization and quality norms will suffer financially, and hospitals whose poor patients have high readmission rates will be penalized. All the while, the “war on waste” will distract policymakers from building the social infrastructure that could lower the high healthcare costs of poverty. These are no ordinary times. For the first time, physicians and their patients are caught in the crosshairs of the “war on waste.”'
So where does this all leave us? The Republicans believe that market forces will help reduce costs and waste while the Democrats look for answers in the Affordable Care Act. What this tells me is that the system is flawed and needs changes which is nothing new. We can't look to politicians for reform as our sole solution. We need to look at the health care system to resolve this.
Monday, November 26, 2012
The Cost of Cancer Care, Part 3
The next topic I will cover is controlling costs in cancer care based on the next article availabe from CancerNetwork.com. Here's a little factoid:
"Cancer patients under active treatment comprise 1% of a payer’s patients but as much as 10% of costs."
Or 'Ouch!'.
Cancer care is expensive. How can the costs be controlled by still providing the patients with the optimal level of care in what is largely still a guessing game? Initial chemotherapy doses are often based on body weight. Then if a patient reacts, the doses can be adjusted down. If one treatmetn doesn't work or has adverse results, then a new treatment is tried. All of which may be very expensive.
Here's a 'brilliant' idea. Have physicians take cost into consideration when prescribing treatment. Well whoop de doo. What about the patient who is the center of all this? They should be the primary consideration.
So then why is cost a consideration? Because costs of treatment are too high and insurance companies are dictating treatment based on their perception of need vs. costs.
"Care for oncology patients, particularly in the adjuvant setting, is often given over predictable time frames. Instead of paying for each element of care separately, episode-of-care payments either can either pay a flat fee per unit of time or a flat fee for a defined care plan. The availability of accepted guidelines in oncology facilitates this payment approach.
Bach et al proposed such a model for metastatic lung cancer.[9] In this model, oncologists would receive a monthly payment derived from the average cost of caring for all patients with metastatic lung cancer. This payment would bundle the costs of chemotherapy, supportive care medications, and administration. Medicare payments would then be adjusted over time based on claims submitted during prior episodes. Physicians would have to demonstrate that treatment conformed to an accepted standard of care. The intent of the program would be to achieve savings by making physicians discretionary purchasers based on price. The downstream effect would also pressure pharmaceutical manufacturers to adjust drug prices downward in order to be economical within the structure of the payment model."
The crux of the problem is cost is so out of proportion to other medical costs that it must be considered for cancer patients. The problem though is the patient's life can depend on the chosen treatment. I like the end result noted above that pharmaceutical manufacturers would need to adjust their pricing. Which is the real goal - make the treatments less expensive - particularly in the US where patients unevenly absorb the research costs that are less frequently distributed to overseas patients.
Another model being reviewed is the Oncology Model Home:
"The medical home model of oncology care is another critical opportunity in the evolving delivery of oncology care, to both ensure quality and reduce cost.[12] The model emphasizes improved care coordination, recognizing that fragmented care acts as an important cost driver in oncology. This model began with the efforts of Dr. John Sprandio with Consultants in Medical Oncology and Hematology, the first oncology practice to achieve level III recognition from the National Committee for Quality Assurance.
The model employs several elements, with its key strength being its synthesis of multiple separate but important efforts in oncology: care coordination, open access, quality measurement, guideline adherence, and cost savings by preventing emergency department (ED) visits and hospitalization. Patient performance status is a key metric for decision-making, including eligibility for chemotherapy administration. This helps to ensure that patients are appropriate for active treatment vs palliative care. Dr. Sprandio’s practice has achieved reductions in ED visits per chemotherapy patient by 68% and hospitalizations per chemotherapy patient by 51%.[13] These are meaningful accomplishments, since the cost of hospitalization may equal or exceed spending on oncology drugs."
I like this idea better. Coordinating care with patient performance as a significant part of the decision making process. This makes the patient the centerpiece as they should be.
Cost containment should never include rationing of care or so called 'death panels' as they are not humane options. In my mind the two issues are costs of care and the patients treatment/quality of life. Any other suggestions are welcome.
"Cancer patients under active treatment comprise 1% of a payer’s patients but as much as 10% of costs."
Or 'Ouch!'.
Cancer care is expensive. How can the costs be controlled by still providing the patients with the optimal level of care in what is largely still a guessing game? Initial chemotherapy doses are often based on body weight. Then if a patient reacts, the doses can be adjusted down. If one treatmetn doesn't work or has adverse results, then a new treatment is tried. All of which may be very expensive.
Here's a 'brilliant' idea. Have physicians take cost into consideration when prescribing treatment. Well whoop de doo. What about the patient who is the center of all this? They should be the primary consideration.
So then why is cost a consideration? Because costs of treatment are too high and insurance companies are dictating treatment based on their perception of need vs. costs.
"Care for oncology patients, particularly in the adjuvant setting, is often given over predictable time frames. Instead of paying for each element of care separately, episode-of-care payments either can either pay a flat fee per unit of time or a flat fee for a defined care plan. The availability of accepted guidelines in oncology facilitates this payment approach.
Bach et al proposed such a model for metastatic lung cancer.[9] In this model, oncologists would receive a monthly payment derived from the average cost of caring for all patients with metastatic lung cancer. This payment would bundle the costs of chemotherapy, supportive care medications, and administration. Medicare payments would then be adjusted over time based on claims submitted during prior episodes. Physicians would have to demonstrate that treatment conformed to an accepted standard of care. The intent of the program would be to achieve savings by making physicians discretionary purchasers based on price. The downstream effect would also pressure pharmaceutical manufacturers to adjust drug prices downward in order to be economical within the structure of the payment model."
The crux of the problem is cost is so out of proportion to other medical costs that it must be considered for cancer patients. The problem though is the patient's life can depend on the chosen treatment. I like the end result noted above that pharmaceutical manufacturers would need to adjust their pricing. Which is the real goal - make the treatments less expensive - particularly in the US where patients unevenly absorb the research costs that are less frequently distributed to overseas patients.
Another model being reviewed is the Oncology Model Home:
"The medical home model of oncology care is another critical opportunity in the evolving delivery of oncology care, to both ensure quality and reduce cost.[12] The model emphasizes improved care coordination, recognizing that fragmented care acts as an important cost driver in oncology. This model began with the efforts of Dr. John Sprandio with Consultants in Medical Oncology and Hematology, the first oncology practice to achieve level III recognition from the National Committee for Quality Assurance.
The model employs several elements, with its key strength being its synthesis of multiple separate but important efforts in oncology: care coordination, open access, quality measurement, guideline adherence, and cost savings by preventing emergency department (ED) visits and hospitalization. Patient performance status is a key metric for decision-making, including eligibility for chemotherapy administration. This helps to ensure that patients are appropriate for active treatment vs palliative care. Dr. Sprandio’s practice has achieved reductions in ED visits per chemotherapy patient by 68% and hospitalizations per chemotherapy patient by 51%.[13] These are meaningful accomplishments, since the cost of hospitalization may equal or exceed spending on oncology drugs."
I like this idea better. Coordinating care with patient performance as a significant part of the decision making process. This makes the patient the centerpiece as they should be.
Cost containment should never include rationing of care or so called 'death panels' as they are not humane options. In my mind the two issues are costs of care and the patients treatment/quality of life. Any other suggestions are welcome.
Sunday, November 25, 2012
The Cost of Cancer Care, Part 2
Cost is now becoming a significant factor in people's cancer treatment decisions - something that should not be happening.
In the past decades, and more significantly in recent years, there have been many developments in cancer treatment. We hear talk about individualized medicine, new treatments which add months to stage IV cancer patients' lives, and more. But we rarely or never hear about the costs. I think of it as the silent side of treatment.
Often these new treatments costs tens of thousands of dollars or more for a single year of treatment with a single dose coming in at the multi-thousand level. What is wrong with this picture? Lots. Why should a patient make a decision on their life because their cancer treatment which could extend their life is out of their price range? Please do not suggest the patients ask for assistance from the pharmaceutical companies because that is not always available.
See this example from an article on CancerNetwork.com, titled "The Cost of Cancer Care, Part I":
"Three years ago, I counseled a patient after a gastrointestinal stromal tumor had been resected from his stomach. I was pleased to be able to tell him that imatinib (Drug information on imatinib) (Gleevec), a drug very well tolerated by most patients, would meaningfully reduce his risk of recurrence. Later, we learned that his out-of-pocket expense under his Medicare Part D plan would be several thousands of dollars for a year of treatment. The patient decided the expense was too onerous and that he would forgo treatment. Patient assistance programs are often limited for Medicare beneficiaries, and none could be secured. I pressed to ascertain whether cost was his sole concern, or if there was another unspoken reason for his resistance to proceed with treatment. There was not; his decision was purely due to cost."
There have been many significant advances in cancer research in recent years including a greater understanding of the biologic side of the disease. The research and FDA approvals can take over a decade to complete. Companies are then offered patent protection for 17 years (or something close to that as my chemo brain fails to recall the exact number) to protect their pricing from competition. Costs in research have escalated creating high drug costs. Other contributing factors are:

The ensuing problem is that costs are high for the patients, insurance companies have high copayments for new non-generic/non-preferred medications. There is a switch to oral treatments which are covered by pharmacy benefits. A chemotherapy infusion may be covered by a $50 copay but an oral chemo in pill form might have a several thousand dollar copay. Its easier on the patient than going to the hospital but much tougher on their wallet. But research has helped saved many lives. There are more gains visible in the coming years as well but at what price?
"These gains have not come without a price. Research and development is expensive. Patients who survive longer under active therapy generally receive more intense overall treatment; this includes not just the therapy itself but also the radiographic and laboratory surveillance necessary to monitor ongoing treatment response and toxicity. While we strive for the development of more effective, less toxic therapies, this progress may be transforming into a painful paradox: the more we advance scientifically, the more constrained we become economically."
So how do we progress and allow advanced treatments, longer lives, and containable costs? That will be part of my next post.
[This is something new for me to have a series looking at a particular issue. As my personal cancer story becomes more of a maintenance factor and a new lifestyle with my other newer ailments, you may see more of these posts in series on differing topics but always ailment related.]
In the past decades, and more significantly in recent years, there have been many developments in cancer treatment. We hear talk about individualized medicine, new treatments which add months to stage IV cancer patients' lives, and more. But we rarely or never hear about the costs. I think of it as the silent side of treatment.
Often these new treatments costs tens of thousands of dollars or more for a single year of treatment with a single dose coming in at the multi-thousand level. What is wrong with this picture? Lots. Why should a patient make a decision on their life because their cancer treatment which could extend their life is out of their price range? Please do not suggest the patients ask for assistance from the pharmaceutical companies because that is not always available.
See this example from an article on CancerNetwork.com, titled "The Cost of Cancer Care, Part I":
"Three years ago, I counseled a patient after a gastrointestinal stromal tumor had been resected from his stomach. I was pleased to be able to tell him that imatinib (Drug information on imatinib) (Gleevec), a drug very well tolerated by most patients, would meaningfully reduce his risk of recurrence. Later, we learned that his out-of-pocket expense under his Medicare Part D plan would be several thousands of dollars for a year of treatment. The patient decided the expense was too onerous and that he would forgo treatment. Patient assistance programs are often limited for Medicare beneficiaries, and none could be secured. I pressed to ascertain whether cost was his sole concern, or if there was another unspoken reason for his resistance to proceed with treatment. There was not; his decision was purely due to cost."
There have been many significant advances in cancer research in recent years including a greater understanding of the biologic side of the disease. The research and FDA approvals can take over a decade to complete. Companies are then offered patent protection for 17 years (or something close to that as my chemo brain fails to recall the exact number) to protect their pricing from competition. Costs in research have escalated creating high drug costs. Other contributing factors are:

The ensuing problem is that costs are high for the patients, insurance companies have high copayments for new non-generic/non-preferred medications. There is a switch to oral treatments which are covered by pharmacy benefits. A chemotherapy infusion may be covered by a $50 copay but an oral chemo in pill form might have a several thousand dollar copay. Its easier on the patient than going to the hospital but much tougher on their wallet. But research has helped saved many lives. There are more gains visible in the coming years as well but at what price?
"These gains have not come without a price. Research and development is expensive. Patients who survive longer under active therapy generally receive more intense overall treatment; this includes not just the therapy itself but also the radiographic and laboratory surveillance necessary to monitor ongoing treatment response and toxicity. While we strive for the development of more effective, less toxic therapies, this progress may be transforming into a painful paradox: the more we advance scientifically, the more constrained we become economically."
So how do we progress and allow advanced treatments, longer lives, and containable costs? That will be part of my next post.
[This is something new for me to have a series looking at a particular issue. As my personal cancer story becomes more of a maintenance factor and a new lifestyle with my other newer ailments, you may see more of these posts in series on differing topics but always ailment related.]
Saturday, November 24, 2012
Costs of Cancer Care
I have decided to do a series on health care costs. A friend sent me a link to an article on the cost of cancer care which is in two parts. And then it had links to more articles so now I am on a roll.
The first article is on healthcare financing and how we pay for our care and insurance. These articles are published on CancerNetwork.com which you will have to join to free of charge to read.
"Fundamental to questions centering on the expense of cancer care in particular and of healthcare in general, is the way in which Americans pay for the healthcare they consume. Most Americans are covered by some type of insurance, and consequently, when they consume healthcare they do not bear the full cost of the care they receive. That is the point of having insurance. We insure against healthcare losses just as we insure our cars and homes against loss.
However, because most private health insurance is an untaxed form of compensation, we spend more on it than we would if it were taxed like other goods and services. This year the tax expenditure, or foregone tax revenues, on employer-provided health insurance is $128 billion. Further, public programs like Medicare and Medicaid are also taxpayer-financed. Altogether, public health insurance and tax-preferred private insurance increase the demand for healthcare relative to the demand that would exist if the programs and more favorable tax treatment had not grown to their current levels.
The point here is that the healthcare advances, the types of technological improvements, and the total spending are all related to the particular financing arrangements that now exist. Though often onerous for patients, out-of-pocket cost-sharing accounts for less than 14% of total personal healthcare spending, while third-party payers account for more than 86%. The out-of-pocket shares for the components of spending on prescription drugs and on physicians are about 19% and 10%, respectively."
So if the true costs of our health care are hidden from us in tax exemptions, tax payer burden, and out of pocket payments, how do we really know what our costs are? I think we all feel our health care costs and national health care spending is too high and out of control. But if we do not even know what our real costs are, how do we cope with it? That is before the collection agencies and bankruptcy courts take away the rest of our money because of the mounting bills.
My feeling is that we need to take a close look at all of the healthcare system and how we pay for treatment, insurance, and absorb the costs of medical advances. This needs to be done systematically and individually. It can no longer be a piecemeal situation where the haves and the have-nots receive different levels of care simply because of what they can or cannot afford.
The first article is on healthcare financing and how we pay for our care and insurance. These articles are published on CancerNetwork.com which you will have to join to free of charge to read.
"Fundamental to questions centering on the expense of cancer care in particular and of healthcare in general, is the way in which Americans pay for the healthcare they consume. Most Americans are covered by some type of insurance, and consequently, when they consume healthcare they do not bear the full cost of the care they receive. That is the point of having insurance. We insure against healthcare losses just as we insure our cars and homes against loss.
However, because most private health insurance is an untaxed form of compensation, we spend more on it than we would if it were taxed like other goods and services. This year the tax expenditure, or foregone tax revenues, on employer-provided health insurance is $128 billion. Further, public programs like Medicare and Medicaid are also taxpayer-financed. Altogether, public health insurance and tax-preferred private insurance increase the demand for healthcare relative to the demand that would exist if the programs and more favorable tax treatment had not grown to their current levels.
The point here is that the healthcare advances, the types of technological improvements, and the total spending are all related to the particular financing arrangements that now exist. Though often onerous for patients, out-of-pocket cost-sharing accounts for less than 14% of total personal healthcare spending, while third-party payers account for more than 86%. The out-of-pocket shares for the components of spending on prescription drugs and on physicians are about 19% and 10%, respectively."
So if the true costs of our health care are hidden from us in tax exemptions, tax payer burden, and out of pocket payments, how do we really know what our costs are? I think we all feel our health care costs and national health care spending is too high and out of control. But if we do not even know what our real costs are, how do we cope with it? That is before the collection agencies and bankruptcy courts take away the rest of our money because of the mounting bills.
My feeling is that we need to take a close look at all of the healthcare system and how we pay for treatment, insurance, and absorb the costs of medical advances. This needs to be done systematically and individually. It can no longer be a piecemeal situation where the haves and the have-nots receive different levels of care simply because of what they can or cannot afford.
Friday, November 23, 2012
Cancer five times
As a cancer patient, what is the worst thing we fear? Being told we have a recurrence or another cancer. So what if between the ages of 29 and 40 something you were told you had cancer five different times? Meet Chef Eric LeVine. He has done this.
I saw him on the Food Network's Chopped a while back and heard him say he had cancer five times. I thought it was significant at the time but not how significant. If you think about it, how many people do you know that have had cancer five times? I spoke at a local senior center last year and a gentleman who had to be in his mid 80's said he had had cancer five times. But he was probably twice the age of Chef LeVine. Its not a common thing.
So Chef LeVine has turned it around and tries to pay it forward by helping family members cope.
"So I realized that the best way for me to use this knowledge - my experience - was to pay it forward. Not with cancer patients, but with their families - teaching them how they can help their family member, the cancer patient."
He talks about people who call constantly 'how are you doing?' and what a drag it is for the patient. It is a constant reminder about cancer and not helping you avoid thinking about it. (Its almost as bad as the people who ask you why you aren't getting the same treatment as their cousin's neighbor's dog walker's hair dresser's uncle who had a different cancer 20 years ago.)
One recommendation I do disagree with him is yes talk to the cancer patient about the crap going on in your life. I would much rather hear someone tell me about their witchy boss, or idiot co-worker, or evil in laws, or annoying children/neighbors, etc than to have them ask me how I am feeling.
However he has been through the cancer roller coaster five times and is still here. I wouldn't want to be in his shoes but he is still here which is the really important part. When I am next in New Jersey, I will make an effort to eat in his restaurant and maybe even meet him.
Subscribe to:
Posts (Atom)